Thank you for visiting ACE Audiology’s Health Downloads section which covers a number of hearing and balance related issues that occur commonly in the community. You can read them online here but you also have the opportunity to download them. Many of the downloads contain links to other authoritative websites should you be seeking secondary sources of information.
The topics shown here are intended to be of benefit to patients, their carers and treating doctors to aid discussion and common understanding. The information contained within this document is general and should not be considered medical advice.
Download Digital Medical Practitioner Audiology Referral Form
We accept referrals in any format and most are by letter. You may however find it convenient to use our editable pdf form. Use the link to open then save to your desktop. The form is quick and easy to complete and can be saved and emailed to ACE Audiology
Fungal otitis externa is known as otomycosis which is most commonly caused by either “Candida albicans” or “Aspergillus niger”. The aetiology of otitis externa is multifactorial however, the common basis is transport of infective material via moisture into the external auditory meatus or secondary to prolonged antibiotic treatment that disturbs the body’s natural flora. Immunosuppression and diabetes may also play a role.
Symptoms
A hearing loss may be evident dependent upon the extent of ear canal occlusion. A blocked or full feeling is apparent and sometimes itchiness, swelling or mild discomfort dependent upon co-existence of bacterial infection. Clients who use hearing devices may indicate the device to be non-functional or to have less volume than previously. Audiometry can be indicative of a conductive loss on the affected side(s) with type B tympanogams and tuning fork tests are likely to be Rinne negative with a lateralized Webber.
Appearance
Occasionally spores may be visible in the external auditory meatus with whitish long filamentous stands of the fungus known individually as hyphae. If the infecting fungus is candida the spores are white. Alternatively if the infecting agent is Aspergillus small black or white balls are evident.
Treatment and Review
Medical practitioners have access to schedule medications that are of high value in treating fungal infection. For ongoing prophylaxis with intact tympanic membranes non prescriptive eardrops such as “AquaEar” are often used by swimmers. Good earmould hygiene is also important in recurring conditions with regular exchange and disposal of domes helpful in removing a source of re-infection. Persistent infection warrants ENT referral by the GP.
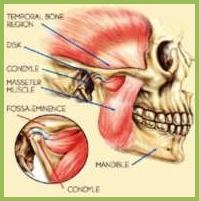
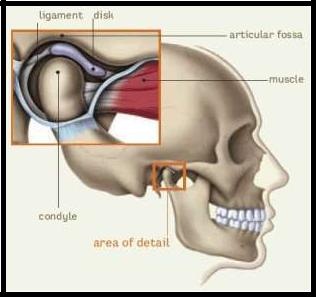
This is a common disorder usually manifested by pain in proximity to the ear and/or the muscles used for chewing affecting about 20% of the adult population.
The condition becomes apparent to Audiologists assessing clients for hearing aids, when the discomfort is reported prior to and sometimes after hearing aid fitting, in and around the ear.
In the absence of obvious explanations for the reported pain the potential of TMJ is usually explored. Often absence of teeth causing an asymmetric chewing pattern is identified. This, combined with a timing mismatch between the left and right mandible upon closing, is a further indication that a TMJ problem may exist.
Sometimes the chewing muscles can be much tenderer on one side than another. Pressing internally on the muscles behind the molar teeth, with a suitable gloved hand, can be further evidence supportive of a TMJ diagnosis,
Discussion with your doctor is advised if you have indications of TMJ. They may consider referring you to an ENT specialist or a Dentist to confirm the diagnosis and to provide appropriate treatment.
In regard to hearing aid fitting the changing of the earmould to soft and pliable materials usually removes the aid as an aggravating factor or indeed switching to a pliable dome acoustic coupling, where feasible, can assist.
Up to 40% of the population will experience dizziness in their lifetime sufficient that advice is sought from a relevant health professional. Vertigo is a sensation of the external environment rotating, leading to imbalance, nausea and at times vomiting. It is usually episodic, passing after a few minutes, and is distinct from “wooziness” or “light-headedness” which can arise from other metabolic factors (e.g. low blood pressure).
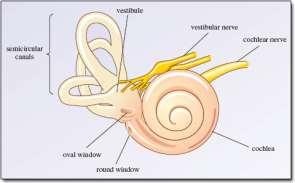
We have two sets of motion detectors (semi-circular canals) in our head that send signals to a central “computer”. When the signals are mismatched such as may be due to loss or damage of a motion detector, then a sensation of vertigo arises.
The motion detectors can be damaged by a large range of insults, inclusive of but not limited to, infection, trauma, stroke and medications. In the event of total loss of a motion detector on one side, within about 7 days central compensation takes place, such that the absent signal is substituted and symptoms decline. The central computer needs to see the mismatch in order for it to build the central compensation required, so inactivity usually leads to a longer recovery period. Vestibular exercises are demonstrated to be highly effective at improving rates of recovery but not all circumstances benefit from this treatment, such as with Benign Paroxysmal Positional Vertigo (BPPV).
Medication can assist initially with acute symptoms but their use delays the natural central compensation processes.
The semicircular canals are responsible for the detection of rotary movement and it is these that are most commonly affected in acute episodes of vertigo. Examination of eye movement, looking for abnormal nystagmus, when gazing in particular directions is helpful in determining which semicircular canal has been affected. As the balance mechanism shares fluid, blood and nerve pathways with the cochlea then hearing aids and examination necessarily forms part of a comprehensive balance assessment.
Benign Paroxysmal Positional Vertigo represents around 50% of vertiginous presentations. The primary causation is a displacement of tiny calcium carbonate crystals used in the balance system to aid detection of movement via their physical mass. These crystals, when misplaced, can be shifted from the posterior canal into a non-disruptive area of the balance mechanism using the Epley manoeuvre. In 80% of cases one treatment is sufficient to successfully treat BPPV.
Vestibular Neuritis arises from an infection damaging the vestibular nerve leading to vertigo and loss of balance. This diagnosis does not benefit from Epley manoeuvres and vestibular rehabilitation is the most effective course forward.
Menieres disease is an episodic vertigo associated with roaring tinnitus and low frequency hearing loss. The duration of vertigo can range from minutes to hours and arises from excess fluid in the inner ear; much like glaucoma is to the eye. In between attacks the individual is usually trouble free of vertiginous symptoms
Migraine can be the causative factor in vertiginous conditions. Often the migraine is “silent’, not associated with pain or other symptoms and its diagnosis is often one of exclusion. Treatment of the migraine and ongoing prophylactic medication to prevent onset are found to be effective means of management of this difficult condition.
Vestibular conditions can be very disturbing to the affected individual, significantly reducing their mobility and capacity to function in their normal daily routine. It is therefore important that the causation is diagnosed to assist in its management. Most vertiginous episodes do resolve but for some they can linger and the expert care of and ENT or Neurologist is advisable.
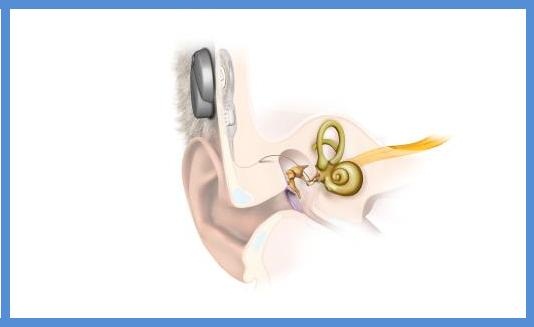
For some individuals the traditional delivery of amplified sound by air conduction is less efficient due to anatomical anomalies or medical conditions. In these situations delivery of sound by bone conduction is an outstanding option providing strong and undistorted sound presentation directly to the inner ear.
Bone Implant systems can be used for the following types of hearing loss:
Conductive Hearing Loss
Mixed Hearing Loss
Single Sided Deafness (Unilateral Dead Ear)
The Med El BonebridgeTMis a fully implantable bone conduction transducer that receives power and data from a small external signal processor that is held in place by magnetism. Alternative technologies use a transcutaneous metal abutment to which the vibrating module is attached externally.
The benefit to the recipient of the implantable device is they are not troubled with the routine of abutment hygiene and the device is more cosmetically appealing with negligible feedback issues.
The Vibrant Soundbridge
The Soundbridge can be used to treat individuals with a mild to moderate degree of sensorineural hearing loss as well conductive and mixed hearing loss, again using implantable technology. It does so by attaching a vibrating transducer on the middle ear ossicles, to add power to the auditory signal, much like a conventional hearing aid does with air conducted sound. It is particularly well suited for individuals for whom conventional hearing aids are contraindicated.
Obtaining Appropriate Audiological and Medical Advice
To determine your Audiological candidature a complex hearing assessment and product evaluation is required. Product evaluations can be simulated with a temporary headband style transducer arrangement. A medical specialist examination will also be required in due course to determine your surgical suitability.
ACE Audiology is able to perform the complex diagnostic assessment, simulator trial, post-operative programming and ongoing aftercare.
Meniere’s Syndrome, also known as, “Endolymphatic Hydrops” is an excess accumulation of endolymph in a cochlear fluid compartment known as Scala Media. It is analogous to glaucoma, whereby excess fluid production or inefficient drainage results in a pressure build up in the eye. The incidence of Meniere’s Syndrome varies between 190 -450 per 100,000 population with a mean age of onset of 43 according to some studies.
Symptoms of Meniere’s Syndrome are a low frequency roaring tinnitus, low tone deafness, aural fullness, vertigo, postural unsteadiness, nausea and vomiting. The low tone deafness and tinnitus symptoms typically increase during an attack. Some studies recommend MRI investigations of the vestibule and cochlea to assess if Endolymphatic Hydrops is present to aid early diagnosis and treatment. A hearing assessment assists greatly in the diagnosis of the disorder particularly when low frequency hearing loss can be demonstrated. The duration of vestibular disturbance is usually 24 minutes to 24 hours and there are multiple recurrences separated by weeks or months of normality. The temporal characteristics assist differentiation between Vestibular Neuritis (acute and non-recurring) and Vestibular Migraine (long duration with history of migraine).
Individuals afflicted with Meniere’s Syndrome initially have to deal with up to three major attacks of vertigo a year with several minor episodes arising as well. As the disease progresses across decades the episodic debilitating vertigo becomes less of an issue with the associated progressive hearing loss tending to be the main difficulty. Speech discrimination ability in Meniere’s affected ears is often worse than would arise from a similar sensorineural loss of other causes. Hearing aids and Meniere’s syndrome requires careful appraisal by the Audiologist and the client needs to be fully aware of what outcomes are most realistic. Hearing aids with memories are often useful as the gain characteristics can be switched dependent upon the state of the diseased ear as may be required for optimal hearing performance
Medical treatment is best managed under specialist guidance. Typical therapies include advice of salt reduced diets, diuretic medication and anti-nausea interventions as required.
For further information and links please select the download. – Menieres_Syndrome.pdf
The onset of tinnitus raises many questions for those affected. Primary amongst those is the matter of causation. Much effort can be expended in seeking an answer and it is only very rarely that a specific disease state is held accountable. Most often no definitive cause can be determined.
What we do know however is that the problem usually originates from damage to the cochlea. By some unknown mechanism the tinnitus is then generated at a neurological level. Some have hypothesized that in the absence of a signal from the damaged part of the cochlea a neurological pathway generates a replacement stimulus much like that of a “phantom limb” pain.
Some evidence for this theory is that the pitch of the tinnitus correlates closely with the part of the cochlea that is most damaged. A central neurological role is also inferred from tinnitus persisting after surgical severance of the acoustic nerve, obviating the cochlea as the generator of the tinnitus.
For most individuals tinnitus is only a mild annoyance and can be dismissed amidst the clatter of daily living, only to be evident in quieter times. Others can however have a severe reaction to their tinnitus and require intervention to assist them to manage the condition.
The sounds we hear do not only connect to the auditory cortex. There are projections to many other parts of the brain. Music, for example, can make you feel sad, relaxed or excited as it impacts upon the emotive parts of our make-up. Importantly some sounds we associate with danger, such as the hissing of a gas pipe or that of a predator is necessary for survival to enable us to escape or defend. Our pulse races and we become agitated. A similar mechanism can be invoked in tinnitus where it is perceived as a threat at a subconscious level creating anxiety and stress just like our inbuilt biological defence systems are intended.
Breaking out of this inbuilt reaction is best managed via a combination of strategies. Informational counselling so that the sufferer has an excellent grasp of the condition, helps build a confidence that there is no danger to be associated with the condition. In addition to counselling use of a masking device is therapeutic. It can give relief from tinnitus under personal control by covering up the tinnitus with a replacement sound that is more palatable. Across time the tinnitus needs to be heard so the sufferer progressively dissociates danger from the perception of their tinnitus.
Long term research has demonstrated that these approaches work well in diminishing the disturbance of tinnitus to manageable levels across a period of several months.
Modern advanced hearing instruments also contain a tinnitus masker in their circuitry that can be turned on or off or up and down by the wearer. As tinnitus is associated with hearing loss the instrument then serves two purposes, one to provide amplification for general hearing and the other therapeutic for the tinnitus distress.
ACE Audiology conducts Tinnitus matching for pitch and loudness, examines outer hair cell function with Otoacoustic Emissions and measures the degree of disturbance after which a customised program of treatment can be discussed with the affected individual.
Benign Paroxysmal Positional Vertigo(BPPV) is the most common form of balance disorderdiagnosed in 40% of cases presenting to health care providers. Fortunately BPPV is relatively simple to diagnose and treat with benefit arising instantly in 80% of interventions. BPPV may recur, however retreatment continues to work effectively.
BPPV Causation
Calcium carbonate crystals, known as otoconia, become displaced from their normal position above the Utricle of the balance organ and enter the Posterior Semi Circular Canal (PSSC). Crystals can enter other semicircular canals but it is the Posterior canal that is mostly involved due to its anatomical predisposition. Head movement in specific planes then induces the displaced otoconia to move within the Posterior Semicircular Canal inducing the sensation of Vertigo and the compensatory eye movements known as nystagmus. BPPV is a mechanical malfunction of the inner ear does not reflect an ongoing disease process.
BPPV Symptoms
Classically, rolling over in bed, laying down or looking up induces the sensation of Vertigo in BPPV. There exists a short latency period after the movement before the vertigo commences. The vertigo crescendos and then fatigues within about 15-45 seconds before the sensation of stability returns.
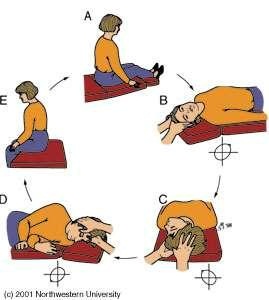
BPPV Diagnosis and Treatment.
BPPV can often be diagnosed on the history alone. The diagnosis can be confirmed by use of the Hallpike Manoeuvre. The Hallpike requires the patient to be moved in a particular manner that placesa load on the Posterior Semicircular Canal to induce vertiginous symptoms as well as permitting an observer to visualize the presence or absence of nystagmus in the patient’s eyes.
The Hallpike Manoeuvre described above is the first step in the treatment process known as the EpleyManoeuvre. It is important that the correct ear is diagnosed so treatment is applied to the affected ear.
Mistreatment can lead to “ear switching” complicating matters. As a consequence, whilst some patients under careful guidance can sometimes manage the Epley Manoeuvre themselves, this is best administered by your treating physician, physiotherapist or audiologist.
ACE Audiology, as well as providing general diagnostic hearing assessment and hearing aid dispensing services, also performs the Hallpike and Epley manoeuvre to diagnose and treat BPPV. Please feel free to contact our clinic on 03 9850 8888 should our services be of interest to you.
Even in the best of times human relationships can experience communication breakdowns. These can be exacerbated if incorrect or disparaging assumptions about the other party’s motivations arise. Now, add to that equation, the misinterpretations that may occur when one of the partners’ experiences hearing loss and the other is in denial!
To facilitate communication repair, Audiologists encourage both partners to attend the hearing assessment and to later join together in the subsequent hearing rehabilitation program. Together the specific communicative difficulties can be determined so work on the solutions can commence.
Firstly it is important that partners understand that for a hearing impaired person the presence of background noise corrupts the communicative process. We know that most hearing impaired individuals require the speech to be ten decibels louder than the surrounding noise. Those with normal hearing can usually cope quite well with speech being 5dB softer than the noise. What this means is that the kettle or dishwasher being turned on will reduce the intelligibility of speech dramatically. Secondly, the loudness of speech diminishes rapidly with distance, so, talking from room to room will no longer be effective. Importantly those sounds that can’t be heard are usually visible on the lips so allowing the hearing impaired person to see your face is particularly important in noisy environments. Sitting opposite each other rather than besides in restaurants provides immediate benefit.
Once these simple concepts are understood it is not difficult to work out why you were understood yesterday but not today. Look carefully at what noise and distances were involved. Re-engineering the acoustics improves communication extraordinarily well. The hearing impaired person must also assume responsibility by seeking clarification by reflecting what was perceived back to the speaker. Expressing interest in what was just said also diminishes the frustration of the speaker who may otherwise assume that the listener is disinterested or disrespectful to their communicative efforts.
Partners can help the process by being frank about the problems they are experiencing in their lives. It is not necessary to rehash who was right or wrong. Shift gears by learning new skills and strategies to make a better life together. The knowledge gained from participating in hearing rehabilitation can go a long way toward improving the broad spectrum of life’s experiences.
Vestibular migraine is the most common form of imbalance occurring in about 1% of the population with a female to male predominance of 5:1. The diagnostic criteria include a diagnosis of migraine, an active migraine disorder, episodic vertigo or imbalance and a time correlation between the symptoms. The time course is quite long in comparison to other balance disorders. The description of imbalance can be vague, sometimes a lightheadedness or as if the floor is moving. Rotational vertigo associated with head movement may be present but is relatively infrequent.
The average age of onset is 38 for females and 42 for males with migraine symptoms predating vertiginous symptoms by some 8 years on average. Benign recurrent vertigo of childhood is likely fitting into this category. Often there exists a family history of migraine, particularly on the maternal line.
Differential diagnosis can be assisted with the appearance of other migraine symptoms such as phonophobia and photophobia (aversion to sound and light respectively), with or without aura. It is not necessary to experience headache pain with the migraine being regarded as “silent”. The duration of imbalance corresponds with the duration of the migraine which can be for hours, days and sometimes weeks, whereas peripheral causations are motion related and/or time limited, in the order of minutes or seconds. Tinnitus and other aural symptoms of hearing and fullness are absent.
Treatment using preventative migraine medications is usually very effective. A time course without recurrence whilst under treatment can be reassuring as to the likely causation. Ongoing prophylactic medication is usually required. Vertiginous Migraineurs are more likely to develop Benign Positional Paroxysmal Vertigo (BPPV) which can be easily diagnosed and treated.
For further information and links please click on the download. – Vestibular Migraine
Vestibular Neuritis is an acute balance disorder that affects 3.5 per 100,000 population and can account for 7% of outpatient’s clinics specializing in the treatment of vertigo, such as the Royal Victorian Eye and Ear Hospital (RVEEH) in Melbourne. Its onset is sudden with intense nausea, vomiting, rotational vertigo, visual disturbance and unstable gait. Tinnitus (ringing in the ears) and a sense of aural fullness can also be present. Often patients will need to confine themselves to bed for at least 3 days and sometimes they will seek hospital admission for unremitting symptoms. By ten days post onset symptoms are significantly reduced. Labyrinthitis is a term reserved to describe involvement of both the balance and hearing organs simultaneously.
Vestibular Neuritis (VN) is the third most common balance disorder behind Vestibular Migraine and Benign Positional Paroxysmal Vertigo (BPPV) and is a costly impost on health services not to mention up to ten days of diminished capacity and mobility of the sufferer.
The causation of VN is considered to be a reactivation of a latent virus in the vestibular apparatus or vestibular nerve ganglia, sometimes around the time of personal stress when it is postulated our immune system is not 100%, or it can be reported as secondary to flu like symptoms. Those afflicted usually start to feel marginally better within the first 24 hours as a process of “cerebellar clamp” commences, reducing the difference in activity between the good and bad ear such that there is less nausea and vertigo. Approaching 72 hours “central compensation” is taking effect in the brain stem to bring the ears to a closer equilibrium and again significantly reducing nausea and vertiginous symptoms.
Recovery Process from Vestibular Neuritis
Time from Onset
Symptoms
Description
First 24 hours
Intense vertigo, nausea and vomiting, gait instability, nystagmus (eyes beating toward the better ear)
One labyrinth is dysfunctional creating a mismatch with the normal ear. Cerebellar clamp commences reducing the resting output rate of the better ear. Anti-nausea and steroidal medication per medical advice
Up to 72 hours
Diminishing symptoms due to treatment and central mechanism’s
“Central Compensation” effective, creating replacement signal in the brainstem to compensate for loss of peripheral signal.
72 hours
Significant reduction in symptoms
Central compensation still in progress
Long Term
Usually symptom free
May be more prone to develop BPPV. Residual imbalance may be due to incomplete compensation for which vestibular rehabilitation can assist
Early medical treatment with anti-nausea medication can alleviate symptoms but conventional advice is for these to be tapered off as prolonged use may delay central vestibular compensation mechanisms. Once the vestibular neuritis episode is over the patient will generally return to a normal life, however there will be likely permanent damage to the vestibular nerve and/or balance organs in the afflicted ear. As we have inbuilt redundancy in our balance organs and central compensation processes in place to enable us to continue functioning there is rarely any significant disablement in future years.
After recovery, clinically it can be difficult to detect the patient has a damage vestibular system. A vestibular assessment can inform which semicircular canals (horizontal, anterior, posterior) and otolith organs (Utricle and Saccule) have been affected permanently and to what extent. This information, due to anatomical connections, infers which branch of the vestibular nerve has been affected.
Post recovery there may be occasional imbalance and veering to one side but usually this is self-correcting due to the wonders of cerebellar functioning. An ear that has suffered Vestibular Neuritis is more prone to develop Benign Paroxysmal Positional Vertigo (BPPV) which can be treated easily and successfully with an Epley maneuver.
This brief educative tool will be of benefit to patients, their carers and treating doctors to aid discussion and common understanding. The information contained within this document is general and should not be considered medical advice. Please consult your doctor should you have concerns about sudden hearing deterioration. Doing so promptly is important to facilitate the best prospects of recovery.
Sudden Sensorineural Hearing Loss
An occurrence of Sudden Sensorineural Hearing loss (SSHL) can be distressing for the affected individual. Patients often report they had a sudden loss most often in one ear when waking in the morning, associated with tinnitus in about 70% of cases and some mild disequilibrium. There is usually an absence of pain, discharge, vesicles or neurological signs.
The typical definition of SSHL is a sensorineural deterioration of 30 decibels across 3 adjacent frequencies (i.e. not wax occlusion or middle ear infection which are conductive in nature). It is most commonly unilateral but can be bilateral.
Audiologists note individuals with long standing asymmetric hearing levels have tendencies for the ears to equalize to equivalent levels of impairment (sensorineural equalization). As such a sudden change might also be a natural progression of the underlying pathology as have been observed over many decades of clinical experience. Simple enquiry may elucidate prior asymmetric hearing levels.
The causation of sudden sensorineural hearing loss is rarely determined and successive studies are not agreed as to the most effective treatment protocol, although steroids appear to be the first line treatment, given promptly after an episode, within 24-48 hours, as per the RVEEH clinical advisory (see download link). Categories of causation have been characterised as autoimmune, vascular, neurologic, trauma/toxin and infections, both viral and bacterial.
General Practitioners may wish to speak with an ENT specialist to obtain expert guidance on the best and current course of intervention. A high priority appointment within 72 hours with an ENT, mediated by the GP, is desirable.
Some studies suggest that up to 65% of patients will experience recovery of their hearing with or without treatment so it is difficult to ascertain if the intervention has any material impact. It is however better to intervene than do nothing.
Audiology can assist chart the extent of deterioration should prior records exist and to chart the progress of recovery. If no recovery is evident the Audiologist can assist with amplification refinements or propose a hearing aid fitting to assist with the communicative deficit.
MORE INFORMATION
Please to continue to download our PDF in which further valuable links from medical practitioners and patients are available. – Sudden Sensorineural Hearing Loss.pdf
ACE Audiology will contact you within 24 hours to confirm your preferred time availability or arrange a suitable alternative *Appointment requests submitted on a weekend will be answered on the Monday